ABC Heart Fail Cardiomyop 2023; 3(1): e20230020
Peripartum Cardiomyopathy
Walkiria Samuel Ávila
![]() , Regina Coeli Marques de Carvalho
, Regina Coeli Marques de Carvalho
![]()
Abstract
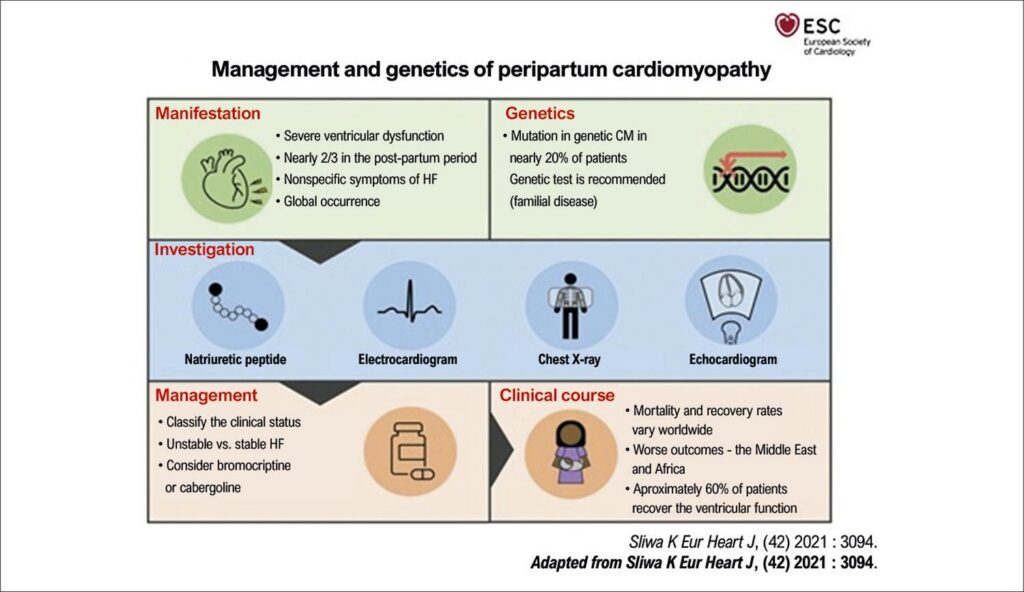
Peripartum cardiomyopathy (PPCM) is a low frequent, but potentially fatal disease, that manifests with heart failure and reduced ejection fraction, with no other identified cause, and related to the puerperal pregnancy cycle. It is a global disease with different clinical manifestations and prognosis. Known risks include preeclampsia, advanced maternal age, multifetal gestation, and African ascendence. Genetic tests have shown that up to 20% of women with PPCM have an identifiable variant of cardiomyopathy. The etiopathogenesis of PPCM, although still unclear, is characterized by endothelial dysfunction caused by anti-angiogenic agents in the placenta, and prolactin degradation products. Clinical manifestation of PPCM does not differ from that of heart failure in other cardiomyopathies, with symptoms varying from mild to cardiogenic shock. Mortality rates in PPCM patients vary widely, and are related to cardiogenic shock, thromboembolism, and complex arrhythmias. The disease may progress rapidly to severe HF, with indication for mechanical circulatory support or cardiac transplant. The treatment of PPCM during gestation is distinct due to potential adverse effects of drugs to pregnancy. However, a careful selection of beta-blockers, diuretics and vasodilators has achieved therapeutic success for the mother and the fetus. Although the treatment meets traditional guidelines developed for nonpregnant adults, the use of bromocriptine (ergot alkaloid) and cabergoline (dopamine D2 receptor agonist) has shown favorable results in ventricular recovery in patients with LVEF < 35% when treated with optimized treatment for heart failure.
Keywords: Cardiomyopathy; Heart Failure; Maternal mortality; Pregnancy
2,788